







- Fact Checked
- March 10, 2026
- 12 min read
Pelvic Floor Pain: Causes, Symptoms, and How to Find Relief

- Written by Daniella Levy • Updated on June 05, 2026
- Updated on June 05, 2026

Table of Contents
Table of Contents
Pelvic pain is surprisingly common, and it can even be expected at certain points in your life, like during pregnancy, after childbirth, or post menopause. But just because something is expected doesn’t mean it needs to be dismissed. Chronic pelvic pain is often more treatable than most people think, and the first step is understanding the root cause.
This post is for informational purposes only and does not constitute medical advice. See full disclaimer below.
What Is the Pelvic Floor?

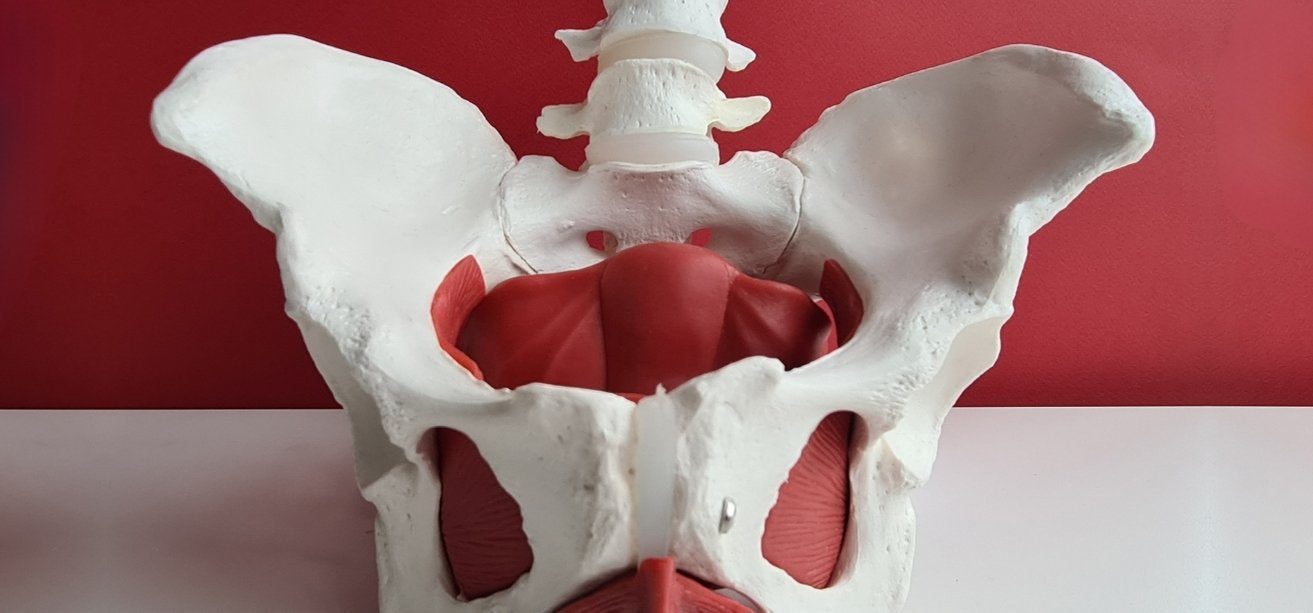
The pelvic floor is an important group of muscles, connective tissue, and nerves that don’t get a whole lot of attention until something goes wrong.1 They form a hammock-like structure at the base of your pelvis, and they support important internal organs in that region, like the bladder, uterus, rectum, and urethra. They also play a central role in urination, bowel movements, sexual function, and core stability.
When the pelvic floor muscles are working well, you don't think about them because, honestly, you don’t really have to.2 But when they become too tight, too weak, or start to spasm for whatever reason, the side effects can ripple across your entire pelvic area and, in some cases, interfere with your day-to-day life.
What Does Pelvic Floor Pain Feel Like?

Pelvic pain feels different for different people. For some, it’s sharp and intermittent, and for others, it’s dull and constant.3 Some people feel it in a specific spot in their pelvis, while others feel it more generally.
Knowing that there is such a wide variation in the pain itself, here are some common symptoms that often accompany pelvic pain:
- Chronic pelvic pain in the lower abdomen, pelvis, tailbone, or lower back
- Pelvic pressure or heaviness, like something is bearing down
- Pain during intercourse (dyspareunia) or pain inserting or wearing tampons
- Pelvic floor muscle spasms, which can feel like cramping or tightening deep in the pelvis
- Pain during urination or bowel movements
- Urinary incontinence or urgency aka leaking when you laugh, sneeze, or exercise
- Fecal incontinence or difficulty with bowel control
- Constipation or incomplete bowel emptying
- Bloating and gastrointestinal discomfort
- Pain during gynecological exams
- Vulvodynia or chronic pain or burning on the vulva without a clear cause
- Back pain, particularly in the lower back and tailbone area
Because pelvic floor pain presents so differently, it can help to know the other symptoms to look for.4 Simply describing the pain you’re feeling might lead to misdiagnosis, but giving your doctor the full range of symptoms gives them more to work with and can help them target the right root cause sooner, so you can feel better faster.
The Impact on Quality of Life
For many women, pelvic floor pain doesn't stay in the pelvis. Instead, it affects sleep, sexual function, relationships, work, and emotional well-being.5 Women with pelvic floor disorders frequently report anxiety and depression, not as separate issues, but as natural consequences of living in pain without answers.
Conditions like pelvic organ prolapse, urinary incontinence, and fecal incontinence also carry significant social stigma, which means women often suffer in silence rather than seek help. If that's you know there is nothing shameful about what you're experiencing, and it is not inevitable. Help exists, and you deserve access to it.
Pelvic Floor Pain During Pregnancy and After Childbirth
When we talk about pregnancy and childbirth, a lot of the conversation revolves around things like morning sickness and medicated versus unmedicated births, but pelvic floor pain is a common symptom of both, and one that many women are blindsided by.6 You don’t have to be.
During pregnancy, the growing uterus puts increasing pressure on the pelvic muscles and connective tissue, leading to pain.7 More than that, hormonal changes also cause ligaments in the area to relax in preparation for childbirth, which can lead to instability and more pain.
During pregnancy, pelvic floor pain most commonly shows up as pelvic girdle pain, which many women describe as a sharp or aching sensation in the lower abdomen, tailbone, or inner thighs that worsens with walking, climbing stairs, or turning over in bed. Some women also experience pelvic pressure and heaviness as the baby descends.8
After childbirth, pelvic floor dysfunction is extremely common.9 Dysfunction can happen whether you deliver vaginally or via C-section, but it’s most common with prolonged pushing, a large baby, or instrumental delivery, as these are more likely to stretch, tear, or weaken pelvic muscles. This dysfunction often manifests as urinary incontinence, fecal incontinence, pelvic organ prolapse, and chronic pelvic pain, which all sound pretty uncomfortable. And make no mistake, it is. But it’s also highly treatable, and your OB/GYN can help you get on the road to recovery. You just have to be brave enough to let them know how you’re feeling during your follow-up appointments.
Other Causes and Risk Factors

While pregnancy and childbirth are the most common causes of pelvic floor pain, they're far from the only ones.10 Other causes of pelvic floor pain can be diverse and include musculoskeletal, gynecologic, and gastrointestinal factors.
The most common musculoskeletal and lifestyle causes of pelvic pain include:
- Muscle tension and trigger points from stress, poor posture, or overuse
- Heavy lifting without proper core engagement, which puts strain on pelvic muscles
- Chronic constipation and straining during bowel movements
- Chronic coughing, which repeatedly engages the pelvic floor under pressure
- Obesity, which increases pressure on the pelvic floor over time
- Sexual trauma, which can cause the pelvic muscles to hold chronic protective tension
- Menopause, when declining estrogen affects the connective tissue and pelvic muscles, contributing to pelvic floor disorders like prolapse and urinary incontinence
And gynecologic and medical causes include:
- Endometriosis. This is one of the most common causes of chronic pelvic pain, where tissue similar to the uterine lining grows outside the uterus, causing inflammation, adhesions, and scar tissue
- Pelvic inflammatory disease (PID), an infection of the reproductive organs that can cause lasting pelvic pain if not treated promptly
- Fibroids or cysts on the uterus or ovaries, which can put pressure on surrounding pelvic muscles and internal organs
- Interstitial cystitis, a chronic bladder condition that causes pelvic pressure and pain often mistaken for recurrent urinary tract infections
- Vaginismus, or involuntary spasming of the pelvic muscles that makes penetration painful or impossible
- Vulvodynia, which is chronic vulvar pain without a clearly identifiable cause
- Pudendal neuralgia, or nerve pain along the pudendal nerve that runs through the pelvic area
If you’re feeling overwhelmed, remember that it’s not up to you to make a diagnosis. Your doctor can help you do that. You just have to know when it’s time to get health and relay all your symptoms openly.
Related Conditions: Why Pelvic Floor Pain Is So Hard to Pin Down
One of the most frustrating things about pelvic floor pain is that it rarely exists in isolation. It can be caused by underlying conditions, triggered by them, or exist alongside them, and the symptoms often overlap so significantly that identifying the pelvic floor as the source of pain can take years.11
And if that wasn’t complicated enough, conditions like endometriosis, pelvic inflammatory disease (PID), and interstitial cystitis genuinely cause pelvic pain.12 But they can also contribute to pelvic floor dysfunction, meaning the original condition and the resulting muscle tension, spasms, or nerve sensitivity both need to be addressed. Treating one without the other is why so many women get partial relief at best.
The bottom line is that if you’ve been diagnosed with one of these conditions but still have unresolved pain, pelvic floor dysfunction may be a missing piece. This means that, along with treating the underlying condition, you may need a referral to a pelvic floor physical therapist or urogynecology specialist to address the pelvic floor specifically.
How Is Pelvic Floor Pain Diagnosed?
While you may alert your doctor to pelvic floor issues during an annual appointment or standard gynecologic checkup, a diagnosis requires a more thorough follow-up workup that typically includes:13
- Sharing your medical history, including your obstetric history, sexual history, and any prior diagnoses
- A physical exam and pelvic exam to assess for tenderness, muscle tension, trigger points, and signs of prolapse or infection
- A musculoskeletal examination, assessing posture, movement, and muscle function to identify contributors outside the pelvis itself
- A rectal exam to assess the pelvic floor muscles internally and evaluate for anorectal involvement
- Urine tests and blood work to rule out infection, hormonal imbalances, or inflammatory conditions
- Pelvic ultrasound to identify fibroids, cysts, or structural abnormalities in the reproductive organs
- Electromyography (EMG) to measure the electrical activity of the pelvic floor muscles and identify dysfunction
- Laparoscopy, a minimally invasive procedure used to diagnose endometriosis, adhesions, and other internal conditions when imaging is inconclusive
- Gastrointestinal specialist referral if bowel symptoms are prominent, a GI workup may help rule out IBS or other contributors
Not every diagnosis requires all these tests, though. And while your doctor can help you determine the best starting point test-wise, it’s good to know all potential testing options so you can advocate for a more comprehensive assessment if you feel like you aren’t being heard or getting the answers you need.14
Treatment Options for Pelvic Floor Pain
Proper diagnosis is important because the reality is, as complicated and far-reaching as pelvic floor pain is, it’s almost always highly treatable.15 The key is matching the treatment to the correct underlying cause.
For most pelvic floor pain, the right treatment isn’t any one thing, but rather a combination of approaches that includes:
Pelvic floor physical therapy

This is the single most effective treatment for pelvic floor pain and dysfunction and involves a specialized physical therapist who uses manual therapy, myofascial release, and trigger point release to address muscle tension, weakness, and coordination problems.16 They'll also teach you pelvic floor stretches, relaxation techniques, and a home program you can do independently.
Many women who enter pelvic floor physical therapy are surprised to learn that the problem isn't a weak pelvic floor that needs more Kegel exercises, but an overactive pelvic floor that needs to learn to release and relax.17 A good pelvic floor PT can tell the difference easily, and your gynecologist or primary care doctor will likely have a recommendation on hand.
Biofeedback
Biofeedback uses sensors to give you real-time information about your pelvic muscle activity, helping you learn to consciously relax or engage muscles that are misfiring.18 It's particularly effective for women with pelvic floor muscle spasms, vaginismus, or urinary incontinence.
Relaxation and mind-body techniques
Because the pelvic floor holds stress and tension the way other muscles do, mind-body approaches can be genuinely therapeutic, not just as coping tools, but as active treatment.19 Deep breathing, guided imagery, meditation, and yoga all help regulate the nervous system and reduce muscle tension. These techniques often work best as part of a broader treatment plan rather than a standalone fix.

Self-care and home practices
Depending on your specific issues, your physical therapist or healthcare provider may recommend:
- Self-massage of the pelvic floor using a crystal wand or dilators to release internal trigger points
- Bladder training to reduce urgency and improve bladder control
- Sleep hygiene habits to support nervous system regulation and pain management
- An anti-inflammatory diet to reduce systemic inflammation that can worsen pelvic pain
- Avoiding foods that can increase inflammation, such as processed foods, refined sugar, and alcohol
Medical treatments
For some women, physical therapy and self-care aren't enough on their own, especially when an underlying condition like endometriosis, prolapse, or chronic pelvic pain syndrome is driving symptoms.20 In those cases, medical intervention becomes part of the treatment plan and may include:
- Pain medications, which may include over-the-counter NSAIDs for acute flares or prescription options for chronic pelvic pain syndrome
- Trigger point injections, or injections of anesthetic or anti-inflammatory medication directly into overactive muscle trigger points
- Pessaries, which are removable devices inserted into the vagina to support pelvic organ prolapse
- Hormonal therapy for pelvic floor changes related to menopause or endometriosis
- Surgical treatments for structural issues like severe prolapse, fibroids, or endometriosis that haven't responded to conservative care
Supporting Your Pelvic Health From the Inside Out
Let’s get one thing straight: supplements won't fix pelvic floor dysfunction on their own, and we'd never suggest otherwise.21 But supporting your overall pelvic environment is a legitimate part of the picture when it comes to combating pelvic pain.
No system of the body is an island, and due to sheer proximity, the vaginal microbiome and the gut microbiome both play a role in pelvic health.22 An imbalanced gut microbiome can contribute to inflammation and gastrointestinal symptoms like bloating and constipation, which can lead to pelvic floor pain, while disruptions in vaginal flora can also cause or compound pain in the area. For women dealing with conditions like endometriosis or pelvic inflammatory disease, systemic inflammation is part of what drives pain, and a healthy microbiome is one factor that supports the body's ability to manage it.
Happy V's Prebiotic + Probiotic is doctor-formulated with clinically studied Lactobacillus strains to support both vaginal and gut health and reduce overall inflammation. It won't treat pelvic floor dysfunction on its own, but as part of a broader approach to pelvic health, supporting your microbiome is a reasonable and low-risk place to start.
Keep the Conversation Going
- Visit our blog for more women’s health tips.
- Join our private Happy V Facebook group to hear from others who’ve been there.
- Explore supplements designed to support your vaginal health journey.
Disclaimer: This blog is for informational and educational purposes only and is not intended to diagnose, treat, cure, or prevent any disease. Statements about supplements have not been evaluated by the Food and Drug Administration. For more information about vaginal infections, visit the CDC or speak to a licensed healthcare provider.


